AUCTORES
Globalize your Research

Research | DOI: https://doi.org/10.31579/2690-1919/188
*Corresponding Author: Anthony Kodzo-Grey Venyo, Department of Urology, North Manchester General Hospital, Delaunay’s Road, Crumpsall, Manchester, Lancashire, M8 5RB, United Kingdom.
Citation: Anthony K. G Venyo, (2021). Hydatid Cyst of the kidney and Ureter: A Review and Update of the Literature. J Clinical Research and Reports, 8(5); DOI:10.31579/2690-1919/188
Copyright: © 2021 Anthony K. G. Venyo. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 28 July 2021 | Accepted: 15 August 2021 | Published: 24 August 2021
Keywords: hydatid cyst; kidney; echinococcal cyst; casoni test; eosinophilia; albendazole; ultrasound scan; computed tomography scan; magnetic resonance imaging scan; peri-cystectomy; partial nephrectomy; nephroureterectomy
Echinococcal (Hydatid) cyst of the kidney is a very uncommon disease which is sporadically reported in Echinococcal endemic areas of the world as well it tends to be reported in non-endemic areas in view of global travel on extremely rare occasions. Hydatid cyst of the kidney could manifest with non-specific symptoms including: loin/flank pain or discomfort; abdominal pain; a mass within the loin or abdomen; hydatiduria; abdominal distension; weight loss; other non-specific symptoms. A history of residence in or having travelled from an echinococcal endemic area and having been in contact with animals including dogs does play an important role in alerting the clinician regarding the possibility of Echinococcal disease is useful. The general and systematic examinations could be normal but tenderness within the loin and tenderness in the upper abdomen could be found which may or may not be associated with a palpable mass within the loin or upper abdomen. The results of routine haematology and biochemistry blood tests could be normal except at times there could be eosinophilia. Urinalysis could show hydatiduria. A positive Casoni intradermal test results or a positive Echinococcal serology test would tend to alert clinicians about Echinococcal disease. Radiology imaging of the abdomen and renal tract including ultrasound scan, computed tomography scan and magnetic resonance scan, of the abdomen would show the cyst (most commonly) or cysts, (occasionally) within the kidney as well the size of the cyst and the amount of normal looking renal parenchyma and presence of daughter cysts could be demonstrated. Furthermore, if there is hydronephrosis or hydroureter the radiology images would reveal it. Treatment of hydatid cyst of the kidney does entail treatment with a combination of:
With regard to outcome a combination of treatment with albendazole and complete excision of the hydatid cyst of the kidney without spillage from the cyst does result in good outcome and no recurrence of the cyst. Occasional recurrence of the hydatid cyst of the kidney has been reported which could perhaps have been due to incomplete excision of the cyst or spillage of the cyst content plus or minus not having taken enough anti-scolicidal agents although some patients had been successfully treated with complete excision of the hydatid cyst alone without antiscolicidal medicament.
Alveolar echinococcosis is a rarely occurring life-threatening disease in human beings [1]. Echinococcal (hydatid) cyst of the kidney is a very rare condition which is caused by the larval stage of Echinococcus granulosus [1-4]. The definitive host for Echinococcus granulosus is stated to be the dog [1]. Ship tends to be the intermediate host for Echinococcus granulosus; however, human beings tend to become accidental intermediate hosts of Echinococcus granulosus [1]. Within the duodenum of a human being, the parasitic embryo does tend to penetrate the duodenal mucosa which then allows access to the blood stream and then enables entry into the liver about 75% of times, the lungs about 15% of times, other organs about 10% of times, isolated or sole involvement of the kidney by hydatid cyst is not common and this tends to constitute 1% to 5% of all Echinococcal (hydatid) cysts in humans [5-8]. It has been iterated that presence of daughter Echinococcal vesicles within urine is considered the only definitive diagnostic sign of Echinococcal disease of the urinary tract; nevertheless, this does occur in 10% to 20% of patients who have Echinococcal disease. [9] The commonest treatment for hydatid cyst of the kidney has mostly been via a surgical option in view of the fact that there is no absolutely effective systemic scolicidal agent. Percutaneous simple aspiration and sclerotherapy injection treatment of cysts of the kidney had tended to be associated with very high rates of recurrence of up to 90% [1,10,11]. Whilst it might be easy for clinicians in Echinococcus endemic area to have a high index suspicion for Echinococcal (hydatid) cyst of the kidney this may not be so easy for clinicians working in areas where Echinococcal disease tends to be hardly encountered. In view of global travel individuals who have moved from Echinococcus endemic areas to non-Echinococcus endemic areas could manifest with symptoms that are attributable to Echinococcal disease including on rare occasions hydatid cyst of the kidney. The following article on Echinococcus (hydatid) cyst of the kidney is divided into two parts (A) Overview and (B) Miscellaneous narrations and discussions related to case reports, case series and studies related to Echinococcus (hydatid) cyst of the kidney.
To review the literature on Echinococcal (hydatid) cyst of the kidney.
Internet data bases were utilized including: Google, Google scholar, Yahoo, and PUBMED. The search words used included: Echinococcus cyst of kidney, Hydatid cyst of kidney. Laparoscopy for renal hydatid disease, surgery for hydatid disease. The article was pivoted upon and updated from a previous publication of the author [12]. Fifty seven references were identified in addition to a previous work of the author that is not available in the internet data base search system which were used to write article which has been divided into two parts: (A) Overview and (B) Miscellaneous narrations and discussions from some case reports, case series and studies related to hydatid cyst of the kidney.
Review of Literature and update of literature
(A) Overview
Definition / General Comments
It has been documented that Hydatidosis or echinococcosis in human beings, is the terminology that is utilized for the zoonotic infection which is caused by larval stages (metacestodes) of cestode species of the genus Echinococcus [13].
Echinococcus granulosus has been stated to be responsible for the causation of hydatid cyst disease [12-14].
Echinococcus multi-locularis has been documented to cause alveolar hydatid cyst [13,14]
Echinococcus vogeli of Echinococcus oligarthrus is said to cause polycystic hydatid disease, a disease which has features of similar to the features of alveolar hydatid disease [13].
It has been iterated that some of the definitive hosts of Echinococcus do include: [14]
Dogs,
Wolves,
Cats,
Or other carnivores.
Intermediate or cystic stages of Echinococcus quite often tend to affect: [14]
Sheep,
Hogs,
Cows,
Rarely man or other mammals.
Some of the documented sites of the body that are affected by Echinococcus include:
Liver – It has been stated that 60% to 70% of Echinococcus infections affect the liver [14].
Brain, [14]
Lung, [14]
The prostate gland – rarely.
Kidney – rarely.
Ureter – rarely.
Testis – rarely.
Spleen – rarely.
Pancreas – rare.
Stomach wall - rare.
Peritoneum – rare.
Bone and or joint (including scapula as well as the humerus, and other bones) – rare.
Ovary – rare.
Uterus – rare.
Cervix – rare.
Soft tissue of lower-limb rare in calf.
Heart and inter-ventricular septum – rare.
Femoral artery – rare and does emanate from thrombus from interventricular septum of the heart.
Eye – rare.
Neck including thyroid gland– rare.
Parotid gland – rare.
Head including the scalp – rare.
Base of skull – rare.
Shoulder.
Areas of high incidence of Echinococcus infection
Areas of high incidence of Echinococcus infection that have been stated do include the ensuing: [13]
East Africa, Spain, Greece, The Middle East, Iran, Western Australia, Chile, Argentina, and Uruguay.
Echinococcus multilocularis has been stated to cause alveolar hydatid disease which often tends to be seen mostly in:
Alaska, Canada, The Soviet Union countries, and Central Europe [13].
Manifestation of hydatid cyst of the kidney.
Hydatid cyst of the kidney could affect adults as well as children. Quite often there would tend to be no history of previous treatment for Echinococcosis; nevertheless, on rare occasions an individual does manifest with a history of having had treatment for Echinococcosis before. Echinococcosis does present with non-specific symptoms and hence a high index of suspicion would be required in order to diagnose the disease. Within the Echinococcus endemic area clinicians might be alert regarding the symptoms and manifestation of the disease but due to global travel on rare occasions Echinococcal disease could be encountered within a non-endemic area for Echinococcus infection. Some of the manifestations of Hydatid disease of the kidney do include: [12]
Flank or loin pain / discomfort – which tends to be a common manifestation.
Abdominal pain – common manifestation.
Incidental finding of mass within the loin or abdomen – a quite common presentation
Hydatiduria – may be the presentation on rare occasions.
Inferior vena cava syndrome may be the presentation in the scenario of obstruction of the inferior vena cava by the disease which does result in bilateral leg oedema, and visible veins on the abdominal wall.
Breathlessness, may be a presentation if there is extension of the hydatid disease into the inferior vena cava up to the right atrium.
Haematuria is uncommon; however, in the scenario of accidental injury to the hydatid cyst of the kidney there could be haematuria.
Weight loss could also be a presenting symptom on rare occasions.
An individual could be diagnosed with a cyst within the kidney a long time ago who did not develop symptoms for many years and the cyst was left alone only to manifest many years subsequently with loin pain or abdominal distension.
Abdominal distension.
Vomiting could on rare occasions occur if the duodenum is obstructed.
Incidental finding of the hydatid cystic lesion in an asymptomatic individual.
Clinical examination findings in cases of hydatid cyst of kidney [12].
The general examination and systematic examination of many patients who have hydatid cyst of the kidney could tend to be normal.
Tenderness within the flank (loin) – there could be tenderness within the loin/flank region.
Tenderness within the upper abdomen – there could be tenderness within the upper abdomen especially within the site of the hydatid cyst (left or right).
A palpable mass within the loin.
A palpable mass in the upper abdomen.
Evidence of abdominal distension may be found.
Laboratory test results
Urine examination [12]
Urinalysis, urine microscopy and culture could be normal with regard to most cases nevertheless, or rare occasions urine microscopy may reveal microscopic features of Echinococcus.
Haematology blood tests [12]
Full blood count and coagulation screen results would generally tend to be normal with regard to cases of hydatid cyst of the kidney; nevertheless, on rare occasions there might be evidence of eosinophilia and in areas of Echinococcus endemic area this would tend to alert clinicians to the possibility of Echinococcal disease.
It has been iterated that eosinophilia tends to be frequently present when there is viable Echinococcal cyst. [14]
Biochemistry blood tests [12]
The results of Serum urea and electrolytes, liver function tests and blood glucose generally tend to be within normal range with regard to patients who have hydatid disease of the kidney but if the results are abnormal this could reflect another disease or condition the patient may be having in addition to hydatid disease of the kidney.
Tests for the diagnosis of Echinococcus granulosus infection
There are antibody tests for Echinococcus infection and it has been documented that serum assays for Echinococcus granulosus are 90% sensitive with occasional false positive results [14].
It has also been iterated that there is high sensitivity and specificity for Echinococcus multilocularis antibody testing [14].
The casoni intradermal skin test has been stated to be associated with 86% true positive rate and hemagglutination test does have positive titres in 80% of patients and these aforementioned tests represent other valuable diagnostic tests [new 15].
The Weinberg reaction which is a complement fixation test was positive in 3 out of 13 patients which did amount to 13% of their patients.
Radiology Imaging
Ultrasound scan [12]
Ultra-sound scan of renal tract, abdomen and pelvis is a common initial radiology imaging investigation of patients who have hydatid cyst of the kidney.
The cyst within the kidney could have multi-septations, the ultra-sound scan would illustrate the size of the cyst in comparison with or relation to the size of any normal residual renal parenchyma. The ultrasound scan would also tend to show if there are cysts within other organs of the abdomen and pelvis or not.
Ultra-sound scan of abdomen and pelvis is a radiology imaging option which could be undertaken during follow-up assessments of patients following their treatment for hydatid disease of the kidney to establish whether or not there is recurrence of hydatid cyst in the follow-up assessment.
Computed tomography (CT) scan [12]
CT scan of renal tract, abdomen and pelvis is a common initial radiology imaging investigation of patients who have hydatid cyst of the kidney.
The cyst within the kidney could have multi-septations, the CT scan would tend to illustrate the size of the cyst in relation to or in comparison with the size of any normal residual renal parenchyma. The CT scan would also show if there are cysts within other organs of the abdomen and pelvis or not.
CT scan of abdomen and pelvis could be undertaken during follow-up assessments of patients who have undergone treatment for hydatid cyst of the kidney to establish whether or not there is recurrence of hydatid cyst in the follow-up assessment.
Majority of hydatid cysts would tend not to show non-contrast enhanced cyst upon CT scanning; nevertheless, contrast-enhancement of a hydatid cyst of the kidney has been reported before.
Magnetic Resonance Imaging Scan [12]
MRI scan of renal tract, abdomen and pelvis is a common initial radiology imaging investigation option for patients who have hydatid cyst of the kidney.
The cyst within the kidney could have multi-septations, the MRI scan would tend to illustrate the size of the cyst in relation to the size of any normal residual renal parenchyma. The MRI scan would also show if there are cysts in other organs of the abdomen and pelvis or not.
MRI scan of abdomen and pelvis could be undertaken during follow-up assessments following their treatment for hydatid disease of the kidney to establish whether or not there is recurrence of hydatid cyst in the follow-up assessment.
Majority of hydatid cysts would tend not to show non-contrast enhanced cyst upon MRI scanning; however, contrast-enhancement of a hydatid cyst of the kidney has been reported before.
Positron Emission Tomography CT (PETCT) Scan [12]
Even though PETCT scan is not a common way of assessing for presence or absence of hydatid cyst of the kidney, if PETCT scan is undertaken for a different reason theoretically the scan could identify a hydatid cyst of a kidney that had been silent incidentally.
Treatment
It has been iterated that generally, surgery tends to be the treatment of choice for hydatid cyst of the kidney [16].
Kidney sparing surgery with removal of the hydatid cyst with peri-cystectomy has been undertaken with regard to75% of cases [16].
It has been stated that nephrectomy has been performed with regard to 25% of cases of hydatid cyst of the kidney and nephrectomy has been reserved for kidneys that have been destroyed by the hydatid disease of the kidney [16].
Very few cases of laparoscopic removal of hydatid cyst of the kidney have been documented to the knowledge of the author and it had been explained that there is fear that the hydatid cyst could rupture and disseminate during the process of dissection, entrapment, and removal of hydatid cyst during the laparoscopy surgery.
The following recommendations have been made relating to the surgical procedures for the removal of hydatid cyst of the kidney:
Utmost care should be taken during the surgical procedure in order to avoid spillage and resulting hydatidosis.
Pre-operative and post-operative one month courses of albendazole should be taken into consideration so as to sterilize the hydatid cyst, decrease the chance of the patient developing anaphylaxis, and to reduce the tension within the cyst wall and that would then lead to reduction in the risk of spillage occurring during the surgical procedure and to reduce the recurrence of hydatid cyst pursuant to the hydatid cyst surgery.
During the procedure of kidney sparing surgery scolicidal solution, for example hypertonic saline should be utilized preceding the opening the cyst cavities to enable killing of the daughter hydatid cysts and hence prevent further spread of hydatid disease or anaphylactic reaction.
Macroscopic Examination Features
Gross examination of a hydatid cyst would tend to demonstrate a large cyst in the kidney with multiple daughter cysts and well as a fibrous peri-capsule when the cyst has been sectioned [12].
Microscopy Examination Features
Microscopy examination of a hydatid cyst of the kidney would tend to illustrate 3 layers of cyst wall as follows: [14]
Innermost layer (germinal layer) which tends to measure 10 to 20 microns, and which does contain nuclei, which gives rise to brood capsules that are attached by short stalk in infectious fertile cysts.
Often with daughter cysts.
Also protoscolices which could be attached or separated with double row of refractile, birefringent, acid fast hooklets which do measure 22 to 40 microns, and 4 round suckers which comprise of hydatid sand.
Daughter cysts could merge and form or provide internal septation to the cyst.
Laminated membrane beneath the germinal layer that tends to be 1 mm thick, avascular, eosinophilic, refractile, and chitinous, and this layer on staining would tend to show positive staining for: PAS and GMS.
Outer layer that tends to be a dense fibrovascular tissue and which does contain chronic inflammatory cells, variable calcification tends to develop more than 5 years later.
On the contrary the microscopy pathology examination features of a hydatid cyst of the kidney could be reported in a summation as follows: [12]
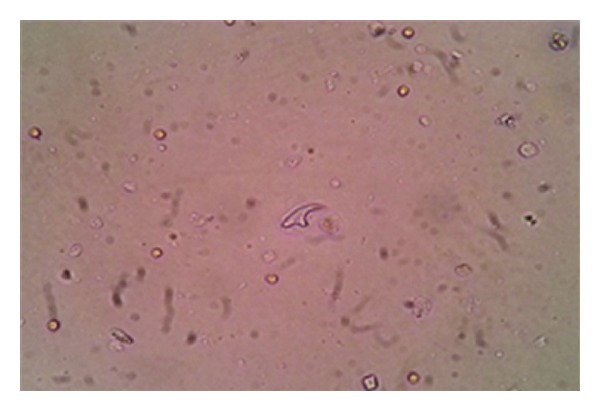
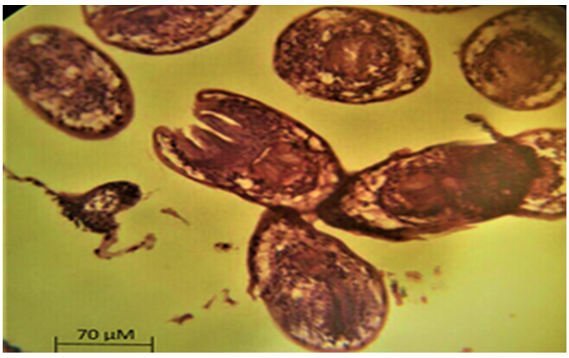
Examination of the cystic fluid would tend to show hooklets and protoscolices of Echinococcus spp.
Histopathology examination showing middle laminated hydatid membranes; granulomatous foreign body reaction and giant multinucleate giant cells surrounding laminary hydatid membrane, as well as renal parenchyma with lesions of chronic pyelonephritis
Differential Diagnosis
Some of the differential diagnosis of hydatid cyst of the kidney do include the ensuing: [12]
Bosniak 2F cyst within the kidney.
Malignant tumour within the wall or segmental wall of a cyst within the kidney.
Malignancy of the kidney.
Ureteropelvic junction obstruction.
Simple cyst of the kidney on rare occasions.
Hydatid cyst of the kidney and ureter could also simulate an urothelial lesion of the ureter with hydroureteronephrosis.
Outcome [12]
Following treatment with cycles of anti-scolicidal medication and surgical excision of the hydatid cyst the prognosis generally tends to be good without recurrent hydatid cyst developing but if a hydatid cyst has been incompletely excised then there would be the possibility of subsequent the development of recurrent hydatid cyst.
In general the utilization of anti-scolicidal agents alone had tended not to completely resolve the hydatid cyst and this had required subsequent surgical excision of the cyst by pericystectomy, partial nephrectomy or nephrectomy; however, with regard to one case report utilization of cycles of albendazole treatment alone had resulted in great reduction in the size of a hydatid cyst of the kidney and the patient had remained asymptomatic for four years and did not require any surgical treatment.
(B) Miscellaneous narrations from some reported cases, case series and studies related to hydatid cyst of the kidney
Akman et al. [17] did report a retrospective review 13 cases of hydatid cyst of the kidney who were treated between 1982 and 1998. They did report that between 1982 and 1998, 13 patients were diagnosed and who had been treated for hydatid cyst of the kidney. Out of the 13 patients 9 were documented to be male and 4 were female and their ages had ranged from 18 years and 65 years and their mean age was 46.8 years. Two of the patients had been admitted because of hydatiduria, and 1 patient had been admitted because of hypertension. Four of the patients did previously undergo surgical exploration for hydatid disease that had involved the liver, kidney, lung, or spleen. Eleven out of the 13 patients were documented to have isolated hydatidosis of the kidney, and two patients were documented to have both liver and kidney hydatid disease. The left kidney was stated to be involved with regard to 4 cases which did amount to 38% of patients, and the right kidney was involved with regard to 9 cases which did amount to 62% of cases. All of the 13 patients had undergone treatment by surgical operation that included: 9 nephrectomies, 1 patient had undergone partial nephrectomy, and 3 patients did undergo excision of their renal cysts. Inferior vena cava injury did occur with regard to 1 case and this was successfully repaired as well as it was found out that that patient had previously undergone surgical operation for hydatid cyst of the liver. The mean follow-up for all of the patients was documented to be four and half years. One of the patients developed re-infestation of the liver by hydatid disease one year pursuant to undergoing kidney surgery for hydatid disease and at that time surgery was performed for the newly developed liver disease. The hydatid cyst which was reportedly confined to the interventricular septum, did develop in one patient who did receive albendazole as adjuvant treatment in addition to undergoing surgical operation. Akman et al. [17] stated the following:
Hydatid disease of the kidney does tend to be an insidious disease, and patients who do have hydatid disease of the kidney quite often do manifest with non-specific symptoms and clinical science.
The common manifestations of hydatid cyst of the kidney do include: dull loin pain, haematuria, hypertension, palpable mass within the flank, and renal colic. Nearly half of their patients which had amounted to 46.2% of their patients had complained of flank pain.
The only pathognomonic sign of hydatid disease of the kidney is hydatid gelatinous material (grape skins, daughter cysts) within the urine (hydatiduria) which is caused by rupture of the hydatid cyst into the collecting system of the kidney [15,18]. With regard to their patients, 2 patients out of the 13 patients that constituted 15.4% of the patients did have hydatiduria and haematuria.
The only abnormality with regard to routine blood tests of patients who have hydatid cyst of the kidney which has diagnostic implications is eosinophilia and this has been reported in 40% to 50% of patients [15,19].
Eosinophilia was found in 5 out of the 13 patients which had comprised of 38.5% of the patients.
The casoni intradermal skin test which does have 86% true positive rate and hemagglutination which does have positive titres in 80% of patients do represent other valuable diagnostic test options [15].
The Weinberg reaction which is a complement fixation test was positive with regard to 3 out of their 13 patients which had amounted to 13% of their patients.
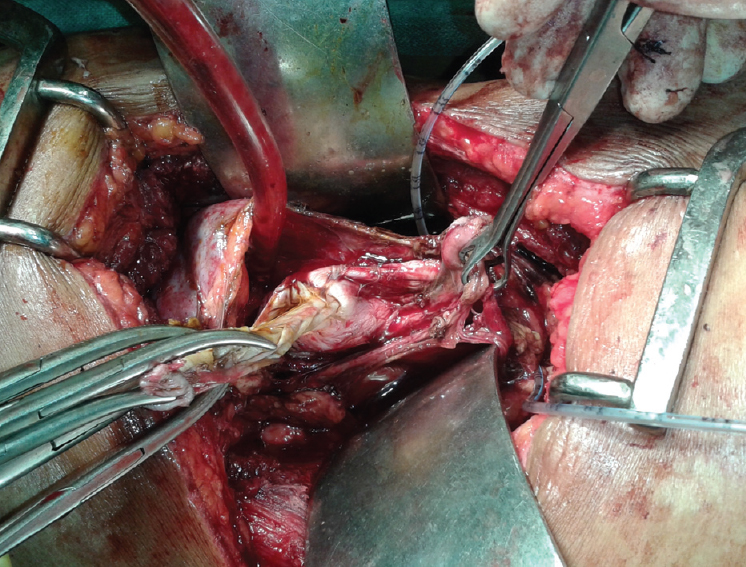
Mongha et al. [16] reported a 21-year-old man who had manifested with a 3-months history of passing intermittently small, white, balloon-like, grape-sized structures within his urine. His general examination and systematic examinations were reported to be normal. No tenderness or palpable mass was found during his abdominal examination, Gross pathology examination of the structure that he passed in his urine revealed a balloon-like structure membranous cyst, which did measure 2 cm. Microscopy histology examination of the cyst had demonstrated an outer laminated layer and an inner germinal layer. The laminated layer did consist of hydatid cyst. His routine haematology and biochemistry blood test results including renal function tests were within normal range as well as there was no evidence of eosinophilia. He had a chest X-ray which was reported to be normal. He had ultrasound scan of abdomen which did demonstrate a multiseptated cyst within his right kidney but the liver was normal. He had computed tomography (CT) scan of the abdomen that revealed a cystic lesion within his right kidney and ureter (see figure 1). The entire right kidney was shown upon the CT scan to have been replaced by the cystic mass. There was no evidence of contrast excretion from the right kidney that was demonstrated upon the CT scan images. He underwent right nephroureterectomy and during the surgical procedure multiple cysts were palpated along the length of his right ureter. He had received albendazole treatment for four weeks preoperatively and he received albendazole treatment for 8 weeks after his right nephroureterectomy operation. Gross pathology examination of the nephroureterectomy specimen did illustrate that the right kidney had been turned into a bag of cysts with multiple daughter cysts within the right ureter (see figure 2). Histopathology examination of the right kidney and right ureter did demonstrate features that been consistent with hydatid cyst of the right kidney and multiple daughter hydatid cysts within the right upper and mid ureter. Mongha et al. [16] stated the following:
Generally, plain radiographs (plain X-rays) tend to be non-specific features and mostly non-revealing of hydatid cysts within the kidney. A thin rim of calcification that delineates a cyst does suggest echinococcal cyst.
Ultrasound scan does help with regards to the diagnosis of hydatid cysts when the daughter hydatid cysts and hydatid sand are shown upon the ultrasound scan imaging. Upon changing the posture of the patient who has hydatid cyst of the kidney under real time, there tends to be shifting of hydatid sand, which could give rise to the “falling snowflake pattern”.
The accuracy of ultrasound scanning with regard to the evaluation of hydatid cyst of the kidney does tend to be operator dependent.
Computed tomography (CT) scan does usually tend to illustrate an expansile, hypo-attenuating tumour that has a well-defined wall and daughter hydatid cysts within the parent hydatid cyst.
CT scan does tend to have an accuracy of 98% and sensitivity to illustrate the daughter hydatid cyst.
Upon CT scan imaging of hydatid cyst of the kidney, the central cystic part of the kidney lesion does tend to have an attenuation of 30 HU to 35 HU which is in contrast to the encompassing cysts that tend to have an attenuation of value of 5 to 15 HU, which does give the mass a wheel-like or rosette appearance.
Magnetic resonance imaging (MRI) scan usually does illustrate a solitary, high-signal-intensity mass which is consistent with multiple thin-walled lesions that is outlined by a thick, hypointense rim. The high signal-intensity has been explained to be due to the characteristic high fluid content of the mass. The small peripheral cysts usually tend to be hypointense in comparison with the central component of the hydatid cyst. MRI scan does demonstrate the cyst adequately; nevertheless, it has been iterated that MRI scan does not have any advantage over CT scan with regard to the diagnosis of hydatid cyst of the kidney [20].


Gupta et al. [21] did report a child who had manifested with left flank swelling and renal colic. She had been having episodes of fever on and off for 2 months. She did have radiology imaging investigations and the features of the radiology images were interpreted to be consistent with the diagnosis of hydatid cyst of the left kidney. She underwent simple left nephrectomy and had continued to be well and without any problems at her 8-months post-operative follow-up.
Rami et al. [22] did report 4 patients who had hydatid cyst of the kidney which were treated between February 2004 and January 2008. The ages of the patients did range between 8 years and 11 years (8 year-old female, 10 year-old female, 11-year-old female, and 10-year-old male). Two of the patients were reported to have double localization of the echinococcal (hydatid) cysts within the kidney and the liver and the other two patients had the echinococcal cyst within the kidney. Radiology imaging which had included ultrasound scan and computed tomography (CT) scan were utilized to establish the diagnosis of the echinococcal cysts. All of the four patients did undergo surgical treatment for hydatid cyst. Two of the patients had standard open surgery. The other two patients had laparoscopic surgery. All four patients did receive albendazole-based treatment for six months post-operatively. All four patients were well at their last follow-up assessments (at 4 years-, 3 years-, 3 years-, 1-year- follow-up).
Fazell et al. [23] reported a 32-year-old man who did manifest with the symptom of vague pain within his left lumbar region over the preceding 3 months. During his examination a mass was found that was palpable within his left lumbar region. His routine haematology and biochemistry blood test results were noted to be within normal range. He had radiology imaging which illustrated a soft tissue mass within the middle part of his left kidney which had measured 115 mm x 130 mm. He did underwent a kidney-sparing peri-cystectomy, and the cyst was removed intact. Histopathology examination of the peri-cystectomy specimen did establish the diagnosis of echinococcal (hydatid) cyst of the left kidney. Fazell et al. [23] iterated that on the whole, surgery tends to be the treatment of choice for hydatid cyst of the kidney and kidney-sparing surgery is regarded the most appropriate treatment for hydatid cyst of the kidney whenever it is possible.
Horchani et al. [5] did report their experience with regard to the management of 147 cases of echinococcal (hydatid) cyst of the kidney over a period of 11 years. They did review the records of 147 patients who had undergone operations for hydatid cyst of the kidney within their institution between 1985 and 1996 in order to address the symptoms of the patients at the time of manifestation, the radiology imaging findings, diagnostic tests that had been undertaken, and the surgical outcomes. Horchani et al. [5] summarized their findings as follows:
All of the patients had undergone surgical treatment.
No pre-operative or post-operative antiparasitic medicament was utilized
Lumbar or lumbo-abdominal pain was the commonest manifestation which was documented with regard to 84% of the cases.
Hydaturia was reported with regard to 28% of the cases.
The pre-operative diagnosis of echinococcal (hydatid) cyst was made based upon findings that were obtained from: intravenous pyelography (IVP), ultrasound scan, and serology tests. Computed tomography (CT) scan was undertaken only in cases of litigation which involved 15% of cases.
With regard to 20 cases, the damage to the parenchyma of the kidney had been so extensive and it had justified performance of nephrectomy.
Abstention did concern 5 involutive type V hydatid cysts.
The rest of the patients had undergone an excision of the prominent part of the cyst (partial cysto-pericystectomy).
The post-operative course of the patients was documented to be smooth with regard to all cases.
Post-operative intravenous pyelogram (IVP) which was performed between 3 months and 6 months pursuant to the surgical operations had shown a restitutio ad integrum (restoration to original condition) in 80% of the cases, and residual distortions of the pelvi-calyceal system with regard to 20% of the cases.
Hochani et al. [5] did conclude that: at the time of publication of their paper the diagnosis of hydatid cyst of the kidney in 2000 had been based mainly upon utilization of ultrasound scan and intravenous pyelogram. Open treatment is the treatment of choice for hydatid cyst of the kidney and it tends to be associated with excellent results.
Seetharami et al. [24] had reported a 37-year-old laboratory technician who manifested with a history of left flank pain and intermittent passage of small, pearly white balloon-like grape sized structures within his urine for the preceding 15 days. He had passed similar structures within his urine a few months earlier. He did have ultrasound scan of his abdomen 18 years earlier and was diagnosed as having a cyst within his left kidney; however, he did not undergo investigation of the cyst further because he was asymptomatic. During his assessment his routine haematology and biochemistry blood test results were noted to be within normal range. He had chest X-ray and abdominal X-ray which were reported to be normal. He had abdominal ultrasound scan which did demonstrate a well-defined cystic lesion which was located within the upper and mid-pole of his left kidney that measured 12 cm x 12 cm which did contain various sizes of multiple cysts and hyper-echoic stroma. He had contrast-enhanced computed tomography (CECT) scan of his abdomen which had illustrated a cystic lesion that measured 11 cm x 13 cm x 13 cm within the upper and mid-pole of his left kidney (see figure 3). The cystic lesion did contain multiple daughter cysts that had given rise to a spoke wheel pattern. The cyst that was observed within the upper and middle pole of his left kidney was associated with left sided hydroureteronephrosis. He did undergo left nephroureterectomy. Pre-operatively, a large thick-walled cyst was observed within the upper and mid pole of the left kidney as well as a thick walled left ureter. The excised specimen did illustrate a large thick walled cyst which did contain many daughter cysts within the kidney and within the upper half of the left ureter. The histopathology examination features of the specimen (see figure 4) was adjudged to be consistent with the diagnosis of hydatid cyst of the left kidney with involvement of the left ureter. Parasitological examination of the cystic fluid had illustrated hooklets and protoscolices of Echinococcus spp. (see figures 5 and 6). His serum did test positive for IgG antibodies which was indicative of the fact that the infection was a long-standing infection. He did receive albendazole for 3 weeks pre-operatively and he also did receive albendazole for 6 weeks pursuant to his surgical operation. He did have an uneventful post-operative recovery.



Bibi et al. [25] did report a 67-year-old woman who did have a history of hydatid cyst of the liver, and who had manifested with dull pain that was ensued by the passage of small, pearly white like structure per urethra on micturition for the preceding 4 months. On examination she was found to have guarding, tenderness as well as a palpable mobile mass within the right upper quadrant of her abdomen. She had ELISA test for Echinococcus antibodies which was found to be positive. She had ultrasound scan of her abdomen which illustrated a multi-vesicular, well defined cystic mass that had extended from the right retroperitoneum to the pelvis where it did appear to be attached to an ectopic kidney. The liver, the spleen and the left kidney were observed to be normal. She had computed tomography (CT) scan of abdomen and the findings had confirmed that the large cyst that measured 15 cm x 12 cm and that it had arisen from the upper pole of her right ectopic pelvic kidney which had replaced the tissue of the kidney. The cyst was observed to be multi-vesicular as well as well-defined and it did have a thin non-enhanced wall which had contained microcalcifications (see figure 7 A). The cyst was found to be close to the uncinate process of the pancreas, the third part of the duodenum and the right colonic hepatic flexure. Within the peri-cyst fat were found inflammatory changes (see figures 7A and 7B). The excretory phase of the CT scan did demonstrate a delayed right renal excretion and calyceal distortion. A diagnosis of isolated Echinococcal (hydatid) cyst of ectopic pelvic kidney was made. She underwent laparotomy which did revealed a cystic mass that had measured 15 cm x and which had covered the entire kidney. Twenty percent (20%) hypertonic saline was injected into the cyst and the encompassing structures were protected by the employment of gauze soaked within hypertonic saline and wrapped around the cyst. A nephrectomy was undertaken after removal of the cyst. Macroscopic pathology examination of the specimen did reveal a large medullar white cyst that contained translucent fluid and various sizes of daughter hydatid cysts. Histopathology examination of the specimen did demonstrate a hydatid cyst which had three layers: (a) an outermost peri-cyst which was fibrous; (b) middle ecto-cyst layer which was laminated, hyaline, and acellular (see figure 8 A); (c) and the inner endo-cyst which is the germinative layer that comprises of the daughter cysts and brood capsules with scolices. It was noted to be associated with granulomatous foreign body reaction (see figure 8 B). The adjacent medullary renal parenchyma did illustrate lesions of chronic pyelonephritis (see figure 8 C). The patient was well at her 6-months post-operative follow-up.

Creative Commons Attribution (CC BY): lets others distribute and copy the article, to create extracts, abstracts, and other revised versions, adaptations or derivative works of or from an article (such as a translation), to include in a collective work (such as an anthology), to text or data mine the article, even for commercial purposes, as long as they credit the author(s), do not represent the author as endorsing their adaptation of the article, and do not modify the article in such a way as to damage the author's honor or reputation.
Creative Commons Attribution-Non Commercial-No Derivs (CC BY-NC-ND): for non-commercial purposes, lets others distribute and copy the article, and to include in a collective work (such as an anthology), as long as they credit the author(s) and provided they do not alter or modify the article.

Creative Commons Attribution (CC BY) which: lets others distribute and copy the article, to create extracts, abstracts, and other revised versions, adaptations or derivative works of or from an article (such as a translation), to include in a collective work (such as an anthology), to text or data mine the article, even for commercial purposes, as long as they credit the author(s), do not represent the author as endorsing their adaptation of the article, and do not modify the article in such a way as to damage the author's honor or reputation.
Creative Commons Attribution-Non Commercial-No Derivs (CC BY-NC-ND): for non-commercial purposes, lets others distribute and copy the article, and to include in a collective work (such as an anthology), as long as they credit the author(s) and provided they do not alter or modify the article.
Demirdag et al. [26] did review the data on 11 patients who had undergone laparoscopic treatment for isolated Echinococcal (hydatid) cyst of the kidney between March 2004 and January 2017. They had examined the demographic characteristics and clinical, laboratory, and radiological findings of cases by the utilization of Mann-Whitney U and t-test in statistical analysis. Demirag et al. [26] summated the results as follows:
The ages of the patients were illustrate to have varied between 25 years and 51 years and the mean age was 36-7 years.
The frequent manifestation of the patients was pain in the lumbar region and in 9 patients a palpable mass was found.
It was found that serological evaluation for Echinococcus granulosus was positive with regard to 5 of the 11 patients.
The sizes of the cyst had ranged between 4 cm and 15 cm and the mean size of the cyst was 7.2 cm.
The operation time for the patients had ranged between 120 minutes and150 minutes and the mean operation time was 128 minutes.
The length of hospital stay did vary between 3 days and 13 days and the mean hospital stay was 4 days.
None of the patients were noted to have developed any peri-operative major complications.
The levels of the haematocrit and creatinine did measure between 26 and 43 with a mean 37.8 for haematocrit and 0.5 to 1.3, with a mean of 0.90 for creatinine in the post-operative period and in comparison these levels were 26 to 45 with a mean of 39 for haematocrit and 0.5 to 1.3 with a mean of 0.9 for creatinine in the pre-operative time. There was no statistically significant difference noted between the pre-operative and post-operative blood test results (P > 055).
The follow-up had varied between 40 months and 166 months and the mean follow-up time was 84 months.
There was no relapse of hydatid cyst documented with regard to in of the patients.
Demirag et al. [26] made the following conclusions and recommendation:
The utilization of the laparoscopic approach for the treatment of hydatid cyst of the kidney is a safe and effective therapeutic option of treatment.
There was no recurrence of hydatid cyst with regard to any of the patients following a long-term period of follow-up.
Further series that includes a large series of patients who have hydatid cyst of the kidney are required.
Uçar et al. [27] did report a 15-year-old young lady who had manifested with abdominal pain. She had ultrasound scan of her abdomen which demonstrated a 3.2 cm x 2.3 cm x 1.9 cm solid mass that contained a cystic component within the lower pole of her right kidney. She had an indirect haemaglutination (IHA) test for Echinococcal granulosus that was reported to be positive with a titre of 1:320 titre. The results of her routine haematology and biochemistry blood tests were within normal range. She received albendazole treatment for 3 months. She did undergo follow-up magnetic resonance (MRI) scan which illustrated a solitary lesion within her right kidney with exophytic extensions that had contained large separations. There was no contrast-enhancement following gadolinium injection. Because there was no regression of the of the right kidney lesion, laparoscopic lower pole right kidney mass cyst excision was undertaken with diode laser. She was hospitalized for 1 day without the need to undergo any blood transfusion. Microscopy histology examination of the specimen demonstrated features that were consistent with hydatid cyst of the kidney. At her 2-months pot-operative follow-up she did have ultrasound scan of renal tract which showed that her kidneys were normal. Uçar et al. [27] made the following conclusions:
Diagnosis of hydatid cyst of the kidney has generally tended to be made incidentally and hydatid cyst of the kidney could be misdiagnosed as a primary kidney tumour.
Radiology imaging studies could prove to be insufficient for the accurate diagnosis of hydatid cyst of the kidney.
With regard to their case, laparoscopic excision of the kidney cyst and histopathology examination of the specimen did confirm the diagnosis of hydatid cyst of the kidney.
With regard to patients who come from echinococcosis endemic areas, hydatid cyst should always be included in the differential diagnosis of cystic masses of the kidney.
Laparoscopic excision of hydatid cysts of the kidney with diode laser is a feasible and safe option of treatment for resistant cases of hydatid cysts of the kidney.
Soares et al. [28] had reported a 14-year-old boy who had a hydatid cyst within the middle third of his left kidney. He had been in contact with dogs, sheep, and goats in his grandparent’s house. He manifested with back pain and haematuria after he had sustained a back injury. He did have ultrasound scan of renal tract and abdomen and pelvis, CT scan of abdomen and pelvis as well as magnetic resonance imaging scan of abdomen and pelvis which did demonstrate presence of hydatid cyst within his left kidney. The diagnosis was confirmed by the support of specific serology test result. He received 4 week cycles of albendazole 400 mg / day, twice per day. This had resulted in progressive reduction with regard to the size of the cyst as well as with regard to a negative Echinococcal serology test. He was hospitalized for 24 days. At his 4-year follow-up, he had remained well and was symptom-free as well as he did have negative disease-specific antibodies, and the cyst had not changed with regard to size from its reduced state. Soares et al. [28] stated that even though the recommended treatment for hydatid cyst of the kidney is surgical excision of the cyst, studies that shown that medical treatment could be an alternative treatment option which would allow for preservation of the kidney.
Shahait et al. [29] did report a 33-year-old man who had manifested with non-specific right flank pain over the preceding 2 years. His urinalysis was documented to be normal. He had a hemagglutinin test which was reported to be positive for hydatid indirect antibodies and his full blood count had shown eosinophilia of 16%. He did have contrast-enhanced computed tomography (CT) scan of thorax, abdomen and pelvis, which demonstrated an 18.8 cm x 15 cm x 16 cm CE3 hydatid cyst of the right kidney which had caused significant mass effect upon the rest of the parenchyma of his right kidney and the adjacent intra-abdominal organs including his liver. He was commenced on a course of albendazole 400 mg twice daily and he did undergo laparoscopy and separation of the structures that were attached to his kidney which contained the cyst and after wrapping gauze which had been soaked with cetrimide around the operation site the cyst as aspirated completely and this yielded 200 ml of fluid. The cyst cavity was injected with 200 millilitres of cetrimide for 15 minutes and the cetrimide was aspirated to empty the cyst cavity. The cyst cavity was filled with another 200 millilitres of cetrimide through injection the second time for 15 minutes following which the cetrimide was completely aspirated and thus emptying the cavity of the cyst to ensure removal of the Echinococcal organs without any spillage. Following this, the cyst was deroofed by carefully peeling off of the peri-cyst to reach the endo-cyst layer which was removed in one piece and then placed in an Endo Catch bag and then removed. Cauterization of the edges of the remaining peri-cyst was undertaken and omental patch was sewn over the operated cyst site. He received 3 cycles of albendazole 10 mg per kilogram daily in two divided doses over a period of 4 weeks that was followed by a week’s rest. He did have a CT scan of thorax, abdomen and pelvis at his 4-month follow-up which did not illustrate any recurrent cyst but it did demonstrate a seroma at the site of surgery which was drained percutaneously. He had remained well up to the time of publication of the case report.
Krieger et al. [30] did report in Russian the development of a disseminated peritoneal lesion after laparoscopic removal of hydatid cyst of the kidney. The details of the article are not available but the case report narration was to highlight the possibility of the development of peritoneal recurrent hydatid lesions on the peritoneum pursuant to an inadvertent or unnoticed spillage of contents of the hydatid cyst of the kidney onto the peritoneum.
Choi et al. [31] reported a 64-year-old woman who was originally from Uzbekistan who had manifested in Korea with left flank pain. She did have computed tomography (CT) scan of her abdomen and pelvis which had illustrated a cystic mass within the upper to middle pole of her left kidney which was initially diagnosed as a malignancy for which she underwent hand-assisted laparoscopic radical left nephrectomy. Macroscopic pathology examination of the specimen illustrated that the mass did comprise of a large unilocular cyst and multiple smaller cysts and no evidence of any grossly visible kidney tissue was visualized. Histology examination of the specimen did confirm that the cystic mass was a hydatid cyst of the kidney. Choi et al [31] made the ensuing concluding statements:
With regard to patients who come from Echinococcus endemic areas, hydatid cyst of the kidney should be included in the differential diagnosis of cystic masses of the kidney that are illustrated in their radiology images.
They had reported a case of hydatid cyst of the kidney in a woman who had migrated from Uzbekistan to Korea.
Aggarwal and Bansal [32] did report three patients who had hydatid cyst of the kidney and who had undergone treatment within their institution between 2008 and 2010. They did report that with regard to all of the 3 patients, the hydatid disease had involved the left kidney but one of the three patients also did have a contemporaneous concomitant involvement of the liver by hydatid cyst. Abdominal pain was noted to be the predominant presenting symptom. A mass was found palpable within the loin with regard to two of the 3 patients. The diagnosis of hydatid cyst of the kidney was confirmed based upon ultrasound scan and computed tomography (CT) scan in all of the three patients. Laparoscopic management of the hydatid cyst of the kidney was completed with regard to 2 cases. A large intrahepatic cyst was encountered with regard to 1 of the patients which prompted conversion of the laparoscopy procedure to an open procedure in 1 case. Aggarwal and Bansal [32] iterated the following:
There are few reports relating to laparoscopic management of hydatid cyst of the kidney.
In their series of 3 patients laparoscopic management of the hydatid cyst of the kidney was attempted in all cases.
The procedures of the treatment did entail laparoscopic aspiration of the contents of the cyst together with sub-total excision of the ectocyst with regard to 2 of the 3 patients and nephrectomy with regard to 1 patient. The latter case of nephrectomy had to be converted from laparoscopy procedure to open surgery in view of the inaccessibility of the hydatid cyst of the liver.
Laparoscopic management of hydatid cyst of the kidney is feasible as well as safe.
Kumar et al. [33] reported their experience with regard to a novel technique which did involve per-cutaneous management of a giant hydatid cyst of the kidney with single-incision laparoscopic assistance. With regard to the method, they did undertake retrograde ureteropyelogram which did not demonstrate any communication between the kidney cyst and the calyceal system. A veress needle was utilized to establish pneumoperitoneum. Three conventional laparoscopic trocas were utilized. Under the guidance of laparoscopy the cyst was punctured. They utilized 10% Povidone-Iodine as the scolicidal solution. The endocyst was removed under vision with utilization of a grasping forceps via the nephroscope. A portex drain was inserted into the cavity of the cyst. Kumar et al. [33] made the following iterations:
Per-cutaneous aspiration and instillation of scolicidal agents ensued by re-aspiration had been described and reported previously. This procedure appears to be attractive in view of its acceptable success rates and reduced morbidity.
With regard to their case, simple aspiration of the cyst would not have been successful due to the fact that the cyst was full of daughter cysts. In addition, a blind percutaneous puncture of the cyst and dilatation could have emanated in perforation of the colon or mesocolon, which quite often does tend to be wrapped over the surface of such giant cysts which would then make laparoscopic guidance and mobilization of the colon a necessary undertaking to do.
Their case was the first documented case of utilization of their technique as well as their technique was minimally invasive and cost effective.
Mercan et al. [34] did report a 29-year-old woman who had an isolated hydatid cyst within the lower pole of her left kidney, who had manifested with of loss of weight and passing cloudy as well as foul-smelling urine. She underwent laparoscopic partial lower polar left nephrectomy during which the cyst was removed en-bloc. She did not develop any post-operative complications and she was discharged on the 5th post-operative day. She did have at her 9-month follow-up computed tomography (CT) scan of abdomen which did not illustrate any recurrent hydatidosis.
Ideally if one can use a serological test to diagnose hydatid disease that would tend to be very helpful. Krige and Beckingham [35] iterated the ensuing:
There are many serology tests that are utilized to diagnose hydatid disease and routine tests to diagnose hydatid disease do include indirect hemagglutination (IHA) test and immunoelectrophoresis (IEP) test.
The sensitivity of IHA in cases of calcified lung lesions tends to be 60% and 88% with regard to peritoneal liver disease with a specificity of 90% to 95%.
IEP has been regarded as a highly specific test; nevertheless, cross reactivity could occur with other infections such as Taenia Solium Cysticercosis) or upon rare occasions in cirrhosis of the liver or in cancer due to cross reactivity with P1 antigen.
More advanced serology tests had been developed with utilization of ELISA test which does have a sensitivity and specificity of 84% and 96.6% respectively, or Western blotting (IB-immunoblot).
There are many diagnostic antigens in IB test. The first antigen to be utilized was 8KDa, which is reported to have a sensitivity and specificity of 91% and 100% respectively [ 4 ]. Many other antigens have been documented that utilize the IB test.
Antigen A (antigen 5) that is composed of two subunits of 38 to 40 and 20 KDa.
The thermostable Antigen B that is composed of 3 antigens of 8 to 12 , 16 and 23 to 24 KDa
The cellular immune response could also be tested by the utilization of a lymphoproliferative assay which is called blast transformation which has been stated to be a very sensitive test utilized to diagnose the disease in seronegative patients.
The Casoni test was described in 1912 by Tomaso Casoni. [36] The Casoni test is an immediate hypersensitivity skin test which is utilized with regard to the diagnosis of hydatid disease. The test does involve the intradermal injection of 0.25 ml of sterilised fluid from hydatid cysts. Human cyst and sterilised by Seitz filtration on the forearm and equal volume of saline injection of the other forearm. Observations are then made for the subsequent 30 minutes and after 1 day to 2 days [36]. A wheal response that occurs at the injection site within 20 minutes is regarded as positive immediate hypersensitivity test result. It has been stated that delayed hypersensitivity reaction usually does read after 18 hours to 24 hours [38]. The test is said to be positive in about 90% of cases of hydatid disease that affects the liver; nevertheless, Casoni test tends to be positive in less than 50% of patients who have hydatid disease elsewhere within the body. It has also been documented that false positive Casoni test results also tend to be common [39]. It has been advised that with regard to Casoni test positivity being a type 1 hypersensitivity reaction, anaphylactic tray should be kept ready before carrying out the Casoni test [40]. In view of this serology tests are rarely generally in use these days [41].
Ray et al. [42] reported a 50-year-old lady who had manifested with right loin pain of 6 months duration. Her general examination and systemic examination were noted to be normal except for tenderness within in her left loin. The results of her routine haematology and biochemistry tests were found to be normal except for eosinophilia. She had ultrasound scan of abdomen and pelvis which demonstrated a 6 cm x 7 cm simple cyst within the parapelvic position of the right kidney and right hydronephrosis (see figure 9 a). She had a contrast-enhanced computed tomography (CT) scan of abdomen and pelvis which demonstrated a large non-communicating cyst of the right kidney that measured 7.93 cm x 6.36 cm x 6,28 cm with a thin rim of smooth wall that compressed the renal pelvis and which had caused right hydronephrosis (see figure 9b). The cyst did not exhibit any contrast enhancement. During surgical exploration of the right kidney, a large cyst was encountered that had extended from the renal hilum to the right renal lower pole which had caused right hydronephrosis. Upon opening the cyst, daughter cysts were visualized. With precaution the cyst fluid was drained, together with all the daughter cysts and the hydatid sands (see figure 10). The ectocyst was dissected from the renal parenchyma. Communication with the pelvicalyceal system was checked by administration of methylene blue through pre-operative placed ureteral catheter. She was treated with albendazole post-operatively. After the treatment there was complete resolution of eosinophilia and she became symptom free. Ray et al. [42] iterated the ensuing:
The terminology “hydatid” had originated from the Greek word “hudatis” which means watery vesicle.
The cystic form of Echinococcus larval stage had been well-recognised from ancient times.
Rudolphi, in 1808, first utilized the terminology hydatid cyst to refer to Echinococcus in human beings [43].

Ameur et al. [44] reported 34 consecutive cases of hydatid cyst of the kidney that had been managed between 1980 and 2001 in 23 men and 11 women whose ages had ranged between 15 years and 73 years with a mean age of 42 years. The clinical manifestations had included pain with regard to 63% of cases, a mass with regard to 26% of cases, hydatiuria with regard to 11.4% of cases, haematuria with regard to 31.4% of cases, prolonged fever with regard to 23% of cases and hypertension with regard to 3% of cases. Intravenous urography was undertaken in all of the patients and this showed calcifications with regard to 5 cases, a mass syndrome with regard to 11 cases, and silent kidney with regard to 2 cases. Computed tomography (CT) scan was undertaken with regard 8 patients and this was necessitated whenever the diagnosis was uncertain, especially with regard to pseudo-neoplastic cysts. Nevertheless, ultrasound scan of abdomen, renal tract, and pelvis did remain the preferred the radiology imaging diagnostic option. The ensuing treatments were undertaken: Resection of the prominent dome was undertaken with regard to 23 cases, peri-cystectomy was undertaken with regard to 5 cases, partial nephrectomy was undertaken with regard to 1 case, and total nephrectomy was undertaken with regard to 6 cases. An associated surgical procedure was undertaken during the same operation which had included liver cyst, and peritoneal hydatid cysts with regard to 3 cases, as well as the operation was deferred due to pulmonary hydatid cyst with regard to 1 case. The post-operative problems that were encountered included: marked urinary fistula with regard to 2 cases and suppuration of the residual cavity in 1 cases which was treated by ultrasound scan-guided aspiration-drainage. Ameur et al. [44] did conclude that the resection of the prominent dome of the kidney was the most adapted treatment whenever it was possible.
Benchekroun et al. [45] reported 45 cases of hydatid cyst of the kidney that were treated over a 20-year period within their institution. The series of cases had included 27 men and 18 women whose ages had ranged between 26 years and 80 years with a mean age of 47 years. The clinical manifestations had included pain with regard to 80% of cases, flank mass with regard to 42% of cases, hydatiuria with regard to 22% of cases, haematuria with regard to 13% of cases, urinary tract infection with regard to 6% of cases, and hypertension with regard to 3% of cases. As part of the investigation of the disease intravenous urography was undertaken with regard to all of the patients and this showed the following: calcifications in the kidney with regard to 35% of cases, renal tumour syndrome with regard to 71% of cases and silent kidney with regard to 22% of cases. .With regard to the surgical approach, a lumbar incision was utilized with regard to regard to 75% of cases, or BARAYA incision with regard to 15% of cases reported. The treatment did entail: cyst roof resections with regard to 18 cases that had amounted to 40%, 6 peri-cystectomies that amounted to 1£%, partial nephrectomy with regard to 2 cases that amounted to 4% of cases, and nephrectomy with regard to 18 cases that amounted to 40% of cases treated. Post-operatively, marked urinary fistula was encountered with regard to two patients and there was one death during the second post-operative month that was related to an associated sarcoma of the kidney. Benchekroun et al. [45] reported this case series as the outcome of their analysis of the epidemiological, pathological, and therapeutic features of hydatid cyst of the kidney which in their opinion did constitute a public health problem in Morocco.
Benchekroun et al. [46] stated that the symptomatology of thirty patients who had hydatid cyst of the kidney they had treated was florid and 83% of the patients had pain, and 43% of the patients had a mass within the flank, as well as 27% the cases had specific symptoms. They had encountered an exceptional case of associated hypertension. With regard to the pre-operative diagnostic radiology imaging investigations, they had utilized ultrasound-scan of abdomen and pelvis and renal tract, and computed tomography (CT) scan of abdomen and pelvis renal tract which had replaced arteriography to a great extent. With regard to the surgical approach to treatment, they had utilized a lumbotomy with regard to 64% of cases, or Baraya incision with regard to 23% of cases which was ensued by treatment of the renal cyst itself and a case of silent kidney on IVU was treated by resection of a protruding dome. Nephrectomy was necessitated with regard to 47% of cases of the kidney lesions. Benchekroun et al. [46] stated that when conservative treatment did appear sufficient the only procedure that was undertaken apart from specific cases, entailed resection of a protruding dome even with regard to scenarios when the hydatid cyst was discharging into excretory pathways. Splenectomy was necessitated with regard to 2 cases out of 22 cases for hydatid cyst of the left kidney. Bechekroun et al. [46] iterated that their case series had emphasized the safety of surgery for hydatid cyst of the kidney in view of only one death that was reported to have occurred 2 months pursuant to the surgical operation in a patient who had an associated sarcoma of the kidney.
Mzali et al. [47] reported 18 patients who had hydatid cyst of the kidney who had undergone surgical intervention from 1982 to 1994. The patients had included 6 men, and 12 women who had a mean age of 38 years and whose ages had ranged between 7 years and 65 years. The commonest symptom was flank pain which occurred with regard to 55% of the patients. Abdominal mass was found upon examination with regard to 38% of the patients. Ultrasound scan was undertaken with regard to all of the patients and this had provided the correct diagnosis with regard to 13 patients that amounted to 72% of the patients. Excretory urography (IVP) was undertaken with regard to 9 of the patients which did show signs of benign tumour process. The surgical procedures that were undertaken were summated as follows: The protruding dome was resected with regard to 12 cases, 1 total nephrectomy was undertaken, 3 partial peri-cystectomy procedures were undertaken, 2 total peri-cystectomy procedures were undertaken, and 1 total nephrectomy was undertaken. There was one post-operative death which amounted to 5.5% of cases and the morbidity involved 11% of the patients. Mzali et al. [47] made the ensuing conclusions:
Hydatid cyst of the kidney is still uncommon but it is possible in endemic areas.
The treatment of hydatid cyst of the kidney usually tends to be surgical and it is still difficult because the treatment procedure should avoid recurrence of hydatid cyst without sacrificing the kidney.
Benjelloun S, et al [48] based upon a series of 45 cases hydatid cysts of the kidney did present a review of the many aspects of this uncommon disease. The mean age of the patients at the time of their initial diagnosis was 30 years with a slight preponderance of females. Hydatid cyst of the kidney did manifest with flank mass in 84% of cases, pain with regard to 73% of cases, and sometimes with a specific presentation with hydatiduria in 29% of cases. Benjelloun et al. [48] emphasized the value of laboratory tests, taking into consideration that the fact that serology tends to be positive in 57% of cases and that ultrasound scan and computed tomography (CT) scan are preferable to arteriography for the diagnosis of hydatid cyst of the kidney. They stated that surgical treatment has been well defined and that lumbar incision tends to be utilized with regard to 60 % of cases treated and anterior incision tends to be used with regard to 40% of cases treated. Conservative surgical treatment does occupy a predominant place in that conservative surgical treatment tends to be undertaken in 84.5% of cases, as resection of the prominent dome tends to be usually sufficient. Benjelloun et al. [48] stated that total nephrectomy should only be considered with regard to the scenario of a completely destroyed kidney which does occur in about 15.5% of cases. They additionally iterated that the post-operative course of the disease generally tends to be uneventful and that re-expansion of the parenchyma of the kidney tends to be observed with regard to 78% of cases which does indicate the benign nature of hydatid cyst of the kidney.
Reza et al. [49] reported a 26-year-old lady who presented with vague abdominal pain. Upon clinical examination she was noted to have a low-blood pressure and to be tender within the left lower quadrant of her abdomen. The results of her haematology and biochemistry blood tests were normal. Her urinalysis revealed a little mucus, epithelial cell and a high amount of red blood cells. She had ultrasound scan of abdomen, pelvis, and renal tract which showed a normal looking right kidney but the left kidney was shown to contain one typical cyst that measured 12.0 cm x 9.3 cm. She had CT scan of abdomen and pelvis which showed the cyst in more details (see figure 11). The reports of the ultrasound scan and CT scan suggested the diagnosis of a left renal cyst to exclude malignancy without a clear or definitive diagnosis. She underwent left renal cystectomy and pathology examination of the specimen confirmed the diagnosis of hydatid cyst of the left kidney (see figure 12 which has demonstrated the protoscoleces of the hydatid cyst) . Her post-operative recovery was uneventful and she was followed-up regularly with routine haematology and biochemistry blood tests as well as ultrasound scan of abdomen and pelvis and renal tract. At her 1-year post-operative follow-up she was well without any recurrent disease.

Figure 12: Tissue section and protoscoleces of hydatid cyst (x 1000 magnification) [49].
Mohamed et al. [50] reported a 48-year-old man who-old Moroccan lady who had manifested with left loin pain which had commenced 2 years earlier. She was asymptomatic otherwise. She was found to be apyrexial. Her general and systematic examination were unremarkable. The results of her urinalysis and routine haematology and biochemistry blood tests were normal. She had ultrasound scan and computed tomography and CT) scan which illustrated a 3-cm cystic lesion which had occupied the mid-zone of her left kidney that had a thickened irregular wall, calcifications, which exhibited partial contrast-enhancement without secondary calcifications, which exhibited partial contrast-enhancement without secondary locations. The radiology imaging investigations did not demonstrate any other abnormalities within the abdomen and pelvis. The kidney lesion based upon its radiology imaging features was diagnosed as cystic renal cell carcinoma (see figure 13). She underwent left trans-peritoneal laparoscopic radical nephrectomy during which the kidney cyst was excised without any spillage of the contents of the cyst or opening of the excretory tracts (see figure 14). Pathology examination of the specimen showed presence of a multi-locular kidney cystic lesion which contained numerous inflammatory cells that had cholesterol clefts (see figures 15, and 16). She was discharged on the third post-operative day to take oral albendazole for 4 weeks. She had undergone regular follow-up assessments that included clinical examinations as well as radiology imaging surveillance during which she had remained well with no evidence of recurrence of hydatid cyst. Mohamed et al. [50] stated the following:
Serology tests can be utilized to confirm results of radiology imaging in cases of hydatid cyst of the kidney [51].
Ultrasound scan imaging, computed tomography imaging, and magnetic resonance imaging tend to be utilized to diagnose as well as evaluated the extent of hydatid cyst of the kidney.
The typical aspect of hydatid cyst of the kidney upon ultrasound scan imaging and computed tomography (CT) scan imaging is the demonstration of a simple cyst with floating membrane or multilocular cyst [52].
With regard to their case ultrasound scan and CT scan demonstrated an atypical cyst that was classified as Bosniak IV according to the modified Bosniak classification of cystic kidney masses. Magnetic resonance imaging (MRI) scan is useful for assessing type IV Bosniak cysts in order to differentiate between pseudo-tumoral hydatid cysts and cystic renal carcinoma but MRI scan could be inconclusive [51].
Lessons that need to be learnt include:
Not all PIRADS 4 renal lesions are malignant tumours because other lesions including hydatid cyst of the kidney could depict PIRADS 4 features upon radiology imaging.
If Urologists and interventional radiologists adopt the option of undertaking radiology imaging biopsies of renal tumours for pathology examination preceding the undertaking of nephrectomies in order to ascertain the pathology diagnosis of the kidney lesion they are treating, the diagnosis of hydatid cyst of the kidney could be established pre-operatively and perhaps individual patients who are found pre-operatively to have hydatid cyst of the kidney can be initially treated pre-operatively with anti-Echinococcus medicaments pre-operatively and assessed whether the renal lesion has resolved and if the lesion has resolved then the undertaking of surgical excision of the kidney lesion could be avoided in some cases.
Mohamed et al. [50] reported a 48-year-old man who-old Moroccan lady who had manifested with left loin pain which had commenced 2 years earlier. She was asymptomatic otherwise. She was found to be apyrexial. Her general and systematic examination were unremarkable. The results of her urinalysis and routine haematology and biochemistry blood tests were normal. She had ultrasound scan and computed tomography and CT) scan which illustrated a 3-cm cystic lesion which had occupied the mid-zone of her left kidney that had a thickened irregular wall, calcifications, which exhibited partial contrast-enhancement without secondary calcifications, which exhibited partial contrast-enhancement without secondary locations. The radiology imaging investigations did not demonstrate any other abnormalities within the abdomen and pelvis. The kidney lesion based upon its radiology imaging features was diagnosed as cystic renal cell carcinoma (see figure 13). She underwent left trans-peritoneal laparoscopic radical nephrectomy during which the kidney cyst was excised without any spillage of the contents of the cyst or opening of the excretory tracts (see figure 14). Pathology examination of the specimen showed presence of a multi-locular kidney cystic lesion which contained numerous inflammatory cells that had cholesterol clefts (see figures 15, and 16). She was discharged on the third post-operative day to take oral albendazole for 4 weeks. She had undergone regular follow-up assessments that included clinical examinations as well as radiology imaging surveillance during which she had remained well with no evidence of recurrence of hydatid cyst. Mohamed et al. [50] stated the following:
Serology tests can be utilized to confirm results of radiology imaging in cases of hydatid cyst of the kidney [51].
Ultrasound scan imaging, computed tomography imaging, and magnetic resonance imaging tend to be utilized to diagnose as well as evaluated the extent of hydatid cyst of the kidney.
The typical aspect of hydatid cyst of the kidney upon ultrasound scan imaging and computed tomography (CT) scan imaging is the demonstration of a simple cyst with floating membrane or multilocular cyst [52].
With regard to their case ultrasound scan and CT scan demonstrated an atypical cyst that was classified as Bosniak IV according to the modified Bosniak classification of cystic kidney masses. Magnetic resonance imaging (MRI) scan is useful for assessing type IV Bosniak cysts in order to differentiate between pseudo-tumoral hydatid cysts and cystic renal carcinoma but MRI scan could be inconclusive [51].
Lessons that need to be learnt include:
Not all PIRADS 4 renal lesions are malignant tumours because other lesions including hydatid cyst of the kidney could depict PIRADS 4 features upon radiology imaging.
If Urologists and interventional radiologists adopt the option of undertaking radiology imaging biopsies of renal tumours for pathology examination preceding the undertaking of nephrectomies in order to ascertain the pathology diagnosis of the kidney lesion they are treating, the diagnosis of hydatid cyst of the kidney could be established pre-operatively and perhaps individual patients who are found pre-operatively to have hydatid cyst of the kidney can be initially treated pre-operatively with anti-Echinococcus medicaments pre-operatively and assessed whether the renal lesion has resolved and if the lesion has resolved then the undertaking of surgical excision of the kidney lesion could be avoided in some cases.
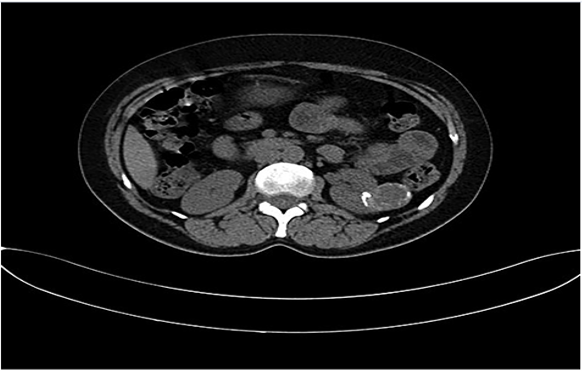

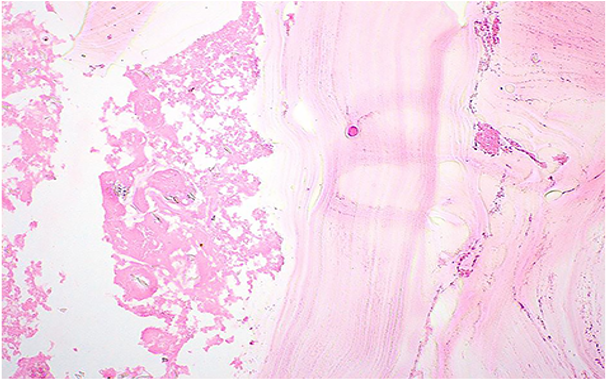
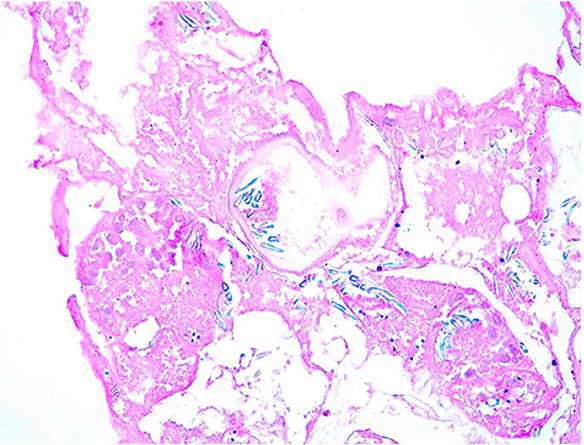
Joyce et al. [53] reported a 12-year-old boy who had a previous history of latent tuberculosis which was treated 10 years earlier and who had manifested with painless visible haematuria over the preceding 2 months. He had occasionally played with local stray dogs. He was asymptomatic otherwise. His general and systematic examinations were normal apart from the fact that his BMI was 35.4 kg/m2. The results of his laboratory blood tests revealed an erythrocyte sedimentation rate (ESR) of 55 mm / hour (normal reference range less than 10 mm per hour). His urinalysis revealed demonstrated erythrocytes and leucocyte esterase. The result of his serology test for HIV was negative and the values of his lymphocyte subset were within normal ranges. He had ultrasound scan of abdomen and pelvis which demonstrated a large irregular echogenic lesion within his left kidney that measured 10 cm. He also had computed tomography (CT) scan of his abdomen which demonstrated an irregular cystic mass that measured 8.2 cm x 8.7 cm x 12.3 cm which had occupied the upper and inter-polar regions of his left kidney. He additionally had magnetic resonance imaging (MRI) of abdomen which demonstrated a heterogeneous centrally necrotic kidney mass which did not exhibit any notable central enhancement. Mild peripheral enhancement of the kidney lesion was visualized upon the MRI scan mass which was considered to have been consistent with fibroinflammatory components. He had CT scan of thorax, and brain which showed many bilateral pulmonary nodules that measured less than 1.2 cm as well as a few clustered ring ring-enhancing lesions within the frontal lobe of his brain than measured equal to / less than 8 mm. He further had MRI scan of brain which demonstrated ring enhancement, together with vasogenic oedema. He had biopsy of his kidney lesion. His CT scan of abdomen also showed an uncommon vascular abnormality of his portal vein system in that his portal veins were diminutive with regard to calibre as well as a large calibre portosystemic shunt which had arisen from his superior mesenteric vein that drained into his right common iliac vein. The abnormality was interpreted to be consistent with a type II congenital portosystemic shunt that is called Abernethy malformation (54). The provisional diagnosis was tuberculosis. Examinations of samples of his sputum, faeces, urine, bronchoalveolar lavage and kidney biopsy did not demonstrate presence of acid-fast bacilli upon staining. The result of mycobacterium tuberculosis PCR test was on the kidney tissue as well as bronchoalveolar lavage were reported to be negative. He was however, commenced on treatment for tuberculosis whilst awaiting the results from his cultures, which were reported to be negative after 6 weeks of incubation. Examination of sections of his core biopsies that were taken demonstrated a predominantly solid lesion that was consisted of dense fibroconnective tissue as well as containing macrophages, myofibroblasts, occasional multi-nucleated giant cells, as well as epithelioid histiocytes. Within a few cores, there was evidence of variable-sized cystic structures encompassed by a thin layer that had a thickness of 17 to 39 micrometres as measured on Masson trichome special stain. The luminal side of the cysts did contain abundant dystrophic calcifications. A scolex was visualized, which was uncommon, and which was suggestive of multi-cystic parasitic mass that had associated peri-parasitic granulomatous, inflammation which was supportive of Echinococcus multilocularis species. Echinococcal species serology test using Echinococcus cyst soluble antigens was strongly positive for Echinococcus infection. A PCR-based assay was undertaken of samples that were sent to the National centre for parasitology was positive for Echinococcus multilocularis infection. He was commenced on Albendazole treatment and the tuberculosis treatment was stopped. His medical treatment was continued and the option of surgical treatment option was deferred due to various reasons including his high BMI which might make the operation of nephrectomy difficult, the presence of his portal shunt, the location and the numbers of the cystic lesions in the kidney and the fear that during the surgical operation there could be rupture of the cysts within the kidney. At his 2-years follow-up, he had remained asymptomatic and he had been tolerating the albendazole treatment. He had been having regular follow-up MRI imaging which had not demonstrated any notable changes with regard to the extent of the kidney lesions. Joyce et al. [53] iterated that their patient had a multi-system disease without evidence of liver involvement in the setting of an uncommon congenital portosystemic shunt. Some of the lessons that had been learnt from this case report include:
On rare occasions, hydatid cysts could affect the kidney as well as other organs without affecting the kidney.
Multiple hydatid cysts can be treated by utilization of medical treatment option that could be associated with good results and control of the infection when it is considered dangerous to undertake nephrectomy or surgical excision of the kidney lesions for various reasons.
Based upon the successful utilization of medicaments to treat multiple hydatid cysts of the kidney it is possible that if the hydatid cysts are localized to one area or two areas of a kidney as in the reported case, a non-invasive procedure of selective renal artery angiography and super-selective embolization of the branch of the renal artery could be undertaken following commencement of anti-echinococcal medicaments but this has not been so far reported in the literature [55].
Reza et al [55] reported a reported a 26-year-old lady resident of Mehdi Abad in Ilam province who had presented with vague abdominal pain, who was referred to the urology department. Her general and systematic examination as well as her urinalysis, routine haematology and biochemistry test results were within normal range. She had ultrasound scan of her renal tract and pelvis and abdomen which showed that the right kidney had measured 12.1 cm and it had a parenchyma thickening of 2.3 cm with no evidence of stone or obstruction; nevertheless, the left kidney had a dimension of 16.5 cm and parenchymal thickness of 1.8 cm, one typical cyst which measured 12.0 cm x 9.3 cm. She had computed tomography scan which showed the details of the cyst (see figure 17). The ultrasound scan of the cyst demonstrated features of a simple kidney which excluded malignancy without any clear diagnosis of the cause of the cyst. She underwent left renal cystectomy and pathology examination of the specimen confirmed features of a definite diagnosis of hydatid cyst as well as proto-scoleces were visualized within the tissue section (see figure 18). She received Albendazole 10 mg / kilogram daily for 12 weeks. She underwent regular follow-up assessments that included ultrasound scan of abdomen, renal tract and pelvis, liver function tests, full blood count and platelet count in order to look out for any cysts and at her 1 year follow-up there was no evidence of recurrence of the hydatid cyst.
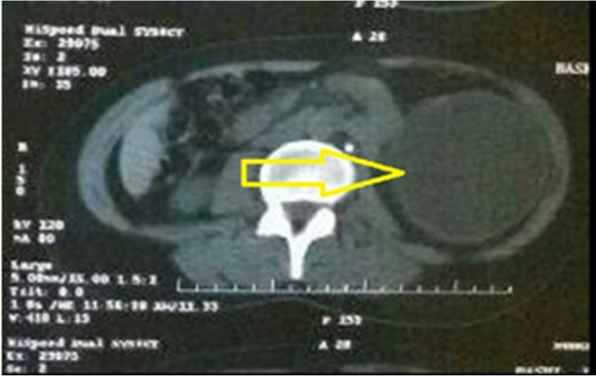
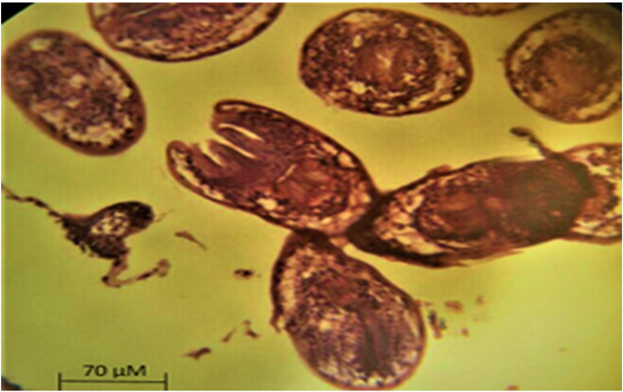
Vuruskan et al. [56] compared the efficacy, safety, and long-term results of laparoscopic and open approaches in patients who undergo surgical treatment for hydatid cysts of the kidney. Vuruskan et al. [56] reviewed the files of 36 patients who had undergone surgical treatment within their clinic based upon the diagnosis of hydatid cyst of the kidney which was confirmed by pathology examination of the specimens. Based upon the surgical technique that was used, the patients were divided into two groups as (open group 1) or laparoscopic (group 2) partial peri-cystectomy. Oral Albendazole 10 mg / kilogram / day in two divided doses for 4 weeks pre-operatively and for three cycles of 4 weeks at 1 week intervals pursuant to the surgical operation in all patients. The demographic characteristics. Laboratory and radiology imaging findings, operation times, hospitalization times, complications, intra-operative bleeding amounts, and recurrence rates had been statistically compared in both groups. The results were summarized as follows:
Open partial peri-cystectomy was undertaken in 21 patients who were assigned to group 1, and laparoscopic trans-peritoneal partial peri-cystectomy was undertaken in 15 patients in group 2.
Operation time and intra-operative bleeding amount in group 1 and group 2 were found to be 19.6 ± 17.1/116.1 ± 17.6 minutes and 125.7 ± 27.8/113.9 ± 19.2 mL, respectively.
There was no statistically significant difference found between the aforementioned values (P = .557, P = .167, respectively).
The duration of hospitalization of both groups was 5.9 ± 1.4/3.6 ± 0.7 days, respectively. The duration of hospitalization in group 2 was statistically significantly shorter (P < .001).
No recurrence developed during the post-operative follow-up in either group.
Vuruskan et al. [56] concluded that in the treatment of hydatid cysts of the kidney, laparoscopy which is a minimally invasive surgical approach, could be technically applied with the same principles as open surgery and it has a similar efficacy and safety profile for short-term and long-term results.
Karami et al. [57] reported a 43-year-old man, who had a history of surgical operation for hydatid cyst of his brain and heart, who had manifested with left-sided chest pain, pain in his left arm, fever, cough, and sputum over the preceding days. He had radiology imaging (ultrasound scan and computed tomography scan0, which demonstrated three cystic lesions within his heart and kidney which had been confirmed by hydatid cyst serology test. Nevertheless, the radiology imaging did not presence of hydatid cyst anywhere else including the liver and the lungs. He refused to undergo any further surgical treatment and he instead opted to receive anti-helminthic treatment. He was commenced on albendazole 400 mg orally twice per day. Karami et al. [57] stated that clinicians should consider the possibility of hydatid cyst when they see evidence of cystic lesions on radiology imaging at uncommon sites for hydatid cysts and hydatid cyst serology tests should be undertaken to exclude hydatid cyst.
Echinococcal (Hydatid) cyst of the kidney alone or with Echinococcal (Hydatid) cyst of the ureter is a disease which clinicians throughout the world must be alert to diagnose in view of world-wide travel, thus a high index of suspicion of the disease needs to be on the mind of each clinician. Eosinophilia could be observed at times in cases of hydatid cyst of the kidney. On rare occasions hydatiduria could be observed. Radiology imaging with the undertaking of ultrasound scan, CT scan, and MRI scan would demonstrate the cyst and quite often the daughter cysts as well. Successful treatment of hydatid cyst of the kidney and ureter would usually tend to include a combination of : (a) anti-scolicidal medicament for example cycles of albendazole and (b) surgical excision of the cyst by laparoscopy or open surgery which may involve pericystectomy or partial nephrectomy for majority of cases of hydatid cyst of the kidney, total nephrectomy for hydatid cysts of the kidney in which almost the entire renal parenchyma have been destroyed and nephroureterectomy for hydatid cysts of the kidney and ureter.
None
Indian Journal of Urology for granting copyright permission for figures and contents of articles from the journal to be reproduced under Copy Right. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Case Reports in Nephrology and Hindawi Journals for granting permission for reproduction and images from Case Reports in Nephrology to be reproduced Copyright © 2012 Venkatesh Seetharami et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Urol. Case Reports and Elsevier under open access document which states that this is an open access journal: After acceptance open access papers will be published under a noncommercial license. For authors requiring a commercial CC BY license, you can apply after your manuscript is accepted for publication. Creative Commons Attribution-NonCommercial NoDerivs (CC BY-NC-ND). For non-commercial purposes, lets others distribute and copy the article, and to include in collective work (such as anthology), as long as they do not alter or modify the article
Annals of Tropical Medicine and Public Health and Medknow Publications for allowing reproduction of figures and contents of their articles under copyright This is an open access Journal and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, to tweak and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms,
Indian Journal of Urology, Case Reports in Nephrology and Hindawi Journals, Urol. Case Reports and Elsevier and Annals of Tropical Medicine and Public Health and Medknow Publications for allowing reproduction of figures from their Journals under the Creative Commons Attribution License, or Creative Commons Attribution-NonCommercial NoDerivs (CC BY-NC-ND). For non-commercial purposes provided the original source is properly cited. The Copy Right to the figures remain under the original source and not this journal.
Oxford Medical Case Reports and Oxford University Press for granting permission for reproduction of contents and figures from their journal article under copy right © 2019 Oxford University Press granted by Oxford University Press through the Copyright Center’s Rights Links This article is available under the Creative Commons CC-BY-NC license and permits non-commercial use, distribution and reproduction in any medium, provided the original work is properly cited. For commercial reuse, permission must be requested.
Journal of Surgical Case Reports and Oxford University Press (OUP) for granting permission for reproduction of figures and contents of their journal article under copyright © 2020, Oxford University Press, which states that This article is available under the Creative Commons CC-BY-NC license and permits non-commercial use, distribution, and reproduction, in any medium, provided the original work is properly cited.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.
